|
Overview
 ?Life begins at 40,? goes an old quote, ?and so do fallen arches.? It?s time to toss that negative idea out the window and get the real facts on fallen arches and what you can do about them. We have all seen what our footprints look like as we walked across sand or left a water trail after getting out of the bathtub. The narrow part of the footprint is where your natural arch exists. What gives you that arch are tendons that pull together to create an upward curve. When your tendons are not properly pulling together, you start to lose that natural arch. This condition is known as flat foot or fallen arch. Causes Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum. Symptoms Pain and stiffness of the medial arch or anywhere along the mid-portion of the foot. Associated discomfort within and near the ankle joint. The knees, hips, and lower back may be the primary source of discomfort. Feet may often feel tired and achy. Painful shin splints may develop with activity. Gait may be awkward. Diagnosis Podiatrists are trained in expertly assessing flat feet and identifying different risk factors and the causes for it. Initial assessment will begin with a detailed history attempting to find out if any underlying illness has resulted in this. A detailed clinical examination normally follows. The patient may be asked to perform certain movements such as walking or standing on their toes to assess the function of the foot. Footwear will also be analysed to see if there has been excessive wear or if they are contributing to the pronation of the foot. To assess the structure of the foot further, the podiatrist may perform certain x-rays to get a detailed idea of the way the bones are arranged and how the muscle tissues may be affecting them. It also helps assess any potential birth defects in a bit more detail. Is flat footedness genetic? Non Surgical Treatment For mild pain or aching, acetaminophen (Tylenol) or a nonsteroidal anti-inflammatory drug (NSAID), such as aspirin or ibuprofen (Advil, Motrin and others) may be effective. Flexible Flatfoot. When there are no symptoms, treatment is not needed. If a child older than age 3 develops symptoms, the doctor may prescribe a therapeutic shoe insert made from a mold of the child's foot or a corrective shoe. As an alternative, some doctors recommend store-bought arch supports. These appear to work as well as more expensive treatments in many children. With any conservative, nonsurgical treatment, the goal is to relieve pain by supporting the arch and correcting any imbalance in the mechanics of the foot. Surgical Treatment  Procedures may include the following. Fusing foot or ankle bones together (arthrodesis). Removing bones or bony growths, also called spurs (excision). Cutting or changing the shape of the bone (osteotomy). Cleaning the tendons' protective coverings (synovectomy). Adding tendon from other parts of your body to tendons in your foot to help balance the "pull" of the tendons and form an arch (tendon transfer). Grafting bone to your foot to make the arch rise more naturally (lateral column lengthening). Prevention It?s time to take a long hard look at what?s in your closet. Now is the time to toss out shoes that are well worn. You also need to say good-bye to thin-soled shoes that offer zero arch support. If you?re overweight, fallen arches may be a sign the universe is trying to tell you something. You need to lose weight, and odds are, fallen arches are but one of many physical discomforts you are experiencing. After Care Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low. Overview
Have you ever been told or noticed that one of your legs is a bit longer than the other? Do you have incidences of lower back pain? These two things could be related. Most individuals have a small difference in their leg lengths. For some, the discrepancy is small and negligible and will not be a contributor to lower back pain. This is usually the case for people if their leg length is less than 5 millimeters. However, a difference of leg lengths greater than 5 millimeters (1/4 inch) can contribute to lower back pain. If you have a leg length difference of greater than 9 mm, then you have a 6X greater likelihood of having an episode of lower back pain. Causes LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio. Symptoms Many people walk around with LLD?s of up to 2 cm. and not even know it. However, discrepancies above 2 cm. becomes more noticeable, and a slight limp is present. But even up to 3 cm. a small lift compensates very well, and many patients are quite happy with this arrangement. Beyond 3 cm. however, the limp is quite pronounced, and medical care is often sought at that point. Walking with a short leg gait is not only unsightly, but increases energy expenditure during ambulation. It could also put more stress on the long leg, and causes functional scoliosis. Where the discrepancy is more severe, walking becomes grotesque or virtually impossible. Diagnosis Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all. Non Surgical Treatment In an adult, we find that we can add a non compressive silicone heel lift to a shoe in increments of 3-4 mm maximum per week. Were we to give a patient with a 20 mm short leg, 20 mm of lift all at once, their entire body would rebel. The various compensations that the body has made, such as curvatures and shortening of muscles on the convex side of the curve, would make such a dramatic change not just noticeable, but painful. When we get close to balancing a patient by lifting a leg with heel inserts, then we perform another gait analysis and follow up xray. At that point, we can typically write them a final prescription to have their shoe modified. A heel lift is typically fine up to 7 mm. When it gets higher than that, the entire shoe must be modified. There are two reasons for this. The back of the shoe is generally too short to accommodate more than 7-8 mm inserted inside the shoes and a heel lift greater than 7 mm will lead to Achilles tendon shortening, which then creates it?s own panoply of problems.  functional leg length discrepancy treatment Surgical Treatment Surgery to shorten the longer leg. This is less involved than lengthening the shorter leg. Shortening may be done in one of two ways. Closing the growth plate of the long leg 2-3 years before growth ends (around age 11-13), letting the short leg catch up. This procedure is called an epiphysiodesis. Taking some bone from the longer leg once growth is complete to even out leg lengths. Surgery to lengthen the shorter leg. This surgery is more involved than surgery to shorten a leg. During this surgery, cuts are made in the leg bone. An external metal frame and bar are attached to the leg bone. This frame and bar slowly pull on the leg bone, lengthening it. The frame and bar must be worn constantly for months to years. When the frame and bar are removed, a leg cast is required for several months. This surgery requires careful and continued follow-up with the surgeon to be sure that healing is going well. Overview
 Plantar fasciitis is a painful condition affecting the bottom of the foot. It is a common cause of heel pain and is sometimes called a heel spur. Plantar fasciitis is the correct term to use when there is active inflammation. Plantar fasciosis is more accurate when there is no inflammation but chronic degeneration instead. Acute plantar fasciitis is defined as inflammation of the origin of the plantar fascia and fascial structures around the area. Plantar fasciitis or fasciosis is usually just on one side. In about 30 per cent of all cases, both feet are affected. This guide will help you understand how plantar fasciitis develops, how the condition causes problems, what can be done for your pain. Causes As stated above, if biomechanical complaints such as over pronation exist during running then this can lead to planter fascitis and heel pain. Over pronation occurs when there is excessive mobility in the sab-taler joint of the foot which causes hyper mobility of the foot. Conditions such as flat feet can also cause over pronation. This increased mobility adversely affects all the muscles in the foot and can even affect the lower leg, upper leg and cause back pain. The mechanical imbalance is highlighted during running due to the increased forces being applied to the body Runners often complain that the pain increases when they enter the toe off phase of the running cycle as this stretches the muscle away from the heel bone. Apart from over pronation, other causes of planter fascitis are a change of running shoes, dramatic increases in speed work, hill work and mileage. Symptoms Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, by being overweight. It doesn't help that fascia doesn't heal particularly quickly because it has relatively poor circulation (which is why it's white in colour). Diagnosis Your doctor will listen to your complaints about your heel and examine you to see what is causing the pain, and whether anything else has started it off. If the cause of your pain seems obvious, your doctor may be happy to start treatment straight away. However, some tests may be helpful in ruling out other problems. Blood tests may be done for arthritis. An Xray will show any arthritis in the ankle or subtalar joint, as well as any fracture or cyst in the calcaneum. (It will also show a spur if you have one, but as we know this is not the cause of the pain.) Occasionally a scan may be used to help spot arthritis or a stress fracture. Non Surgical Treatment Curing posterior heel pain requires calming the inflammation, resting the foot and increasing calf flexibility. Ice therapy and anti-inflammatory medications can be used to reduce the inflammation. Stopping exercises that stress the calf and Achilles is important. This includes walking, running and the use of stair climbers and elliptical machines. Placing a heel lift in each shoe can reduce some of the excess strain on the back of the heel. Stretching exercises to increase calf flexibility are important in curing this problem and preventing its recurrence. Wearing running shoes also provides good foot support and helps with this condition. Sometimes a walking boot is used to immobilize the ankle and let the area completely rest. Physical therapy is sometimes ordered to help reduce the inflammation and pain and to help improve the flexibility of the calf muscles. Occasionally these measures fail to relieve the pain and surgery may be needed. The surgical procedure involves removing bone spurs and repairing any damage to the tendon. Surgical Treatment It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation. heel pads shoes too big Prevention  Flexibility is key when it comes to staving off the pain associated with these heel conditions. The body is designed to work in harmony, so stretching shouldn?t be concentrated solely on the foot itself. The sympathetic tendons and muscles that move the foot should also be stretched and gently exercised to ensure the best results for your heel stretches. Take the time to stretch thighs, calves and ankles to encourage healthy blood flow and relaxed muscle tension that will keep pain to a minimum. If ice is recommended by a doctor, try freezing a half bottle of water and slowly rolling your bare foot back and forth over it for as long as is comfortable. The use of elastic or canvas straps to facilitate stretching of an extended leg can also be helpful when stretching without an assistant handy. Once cleared by a doctor, a daily regimen of over-the-counter anti-inflammatory medication like Naproxen Sodium will keep pain at bay and increase flexibility in those afflicted by heel pain. While this medication is not intended to act as a substitute for medical assessments, orthopedics or stretching, it can nonetheless be helpful in keeping discomfort muted enough to enjoy daily life. When taking any medication for your heel pain, be sure to follow directions regarding food and drink, and ask your pharmacist about possible interactions with existing medications or frequent activities. Overview
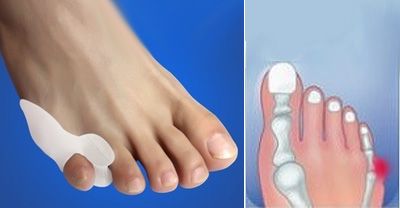
 A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump. A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump.Causes There are orthoses and corrective shoes that can effectively alleviate disturbances to foot mechanics. A podiatric physician can prescribe the best corrective footwear and shoe inserts for all activities, work, exercise, play, walking, shopping and more, based on an analysis of the patient?s foot and his or her lifestyle. Improper footwear. Podiatric physicians have long believed that constricting, narrow, poor-fitting shoes with a tight or pointed toe box tend to compress the end of the foot, leading to abnormal motion of the foot and to excessive pressure in the area of the nerve. High-heeled shoes are a particular culprit here, since they put pressure on the area around wearer?s toes and the ball of the foot. Symptoms What are the symptoms of Morton?s neuroma? A sharp or stinging pain between the toes when standing or walking. Pain in the forefoot between the toes. Swelling between the toes. Tingling (?pins and needles?) and numbness. Feeling like there is a ?bunched up sock? or a pebble or marble under the ball of the foot. Diagnosis Morton?s neuroma can be identified during a physical exam, after pressing on the bottom of the foot. This maneuver usually reproduces the patient?s pain. MRI and ultrasound are imaging studiesthat can demonstrate the presence of the neuroma. An x-ray may also be ordered to make sure no other issues exist in the foot. A local anesthetic injection along the neuroma may temporarily abolish the pain, and help confirm the diagnosis. Non Surgical Treatment Initial treatment for Morton?s Neuroma may include non-prescription anti-inflammatory medications to reduce pain and swelling. These may consist of standard analgesics such as aspirin and ibuprofen (Advil, Motrin, others). Massaging the painful region three times daily with ice. Change of footwear. Avoid tight shoes, high heels or any footwear that seems to irritate the condition. Low heeled shoes with softer soles are preferable. Arch supports and foot pads to help reduce pressure on the nerve. In some cases, a physician may prescribe a customized shoe insert, molded to fit the contours of the patient?s foot. Reducing activities causing stress to the foot, including jogging, dancing, aerobic activity or any high impact movements of the foot. Injections of a corticosteroid medication to reduce the swelling and inflammation of the nerve and reduce pain. Occasionally other substances may be injected in order to ?ablate? the Neuroma. (The overuse of injected steroids is to be avoided however, as side effects, including weight gain and high blood pressure can result.) 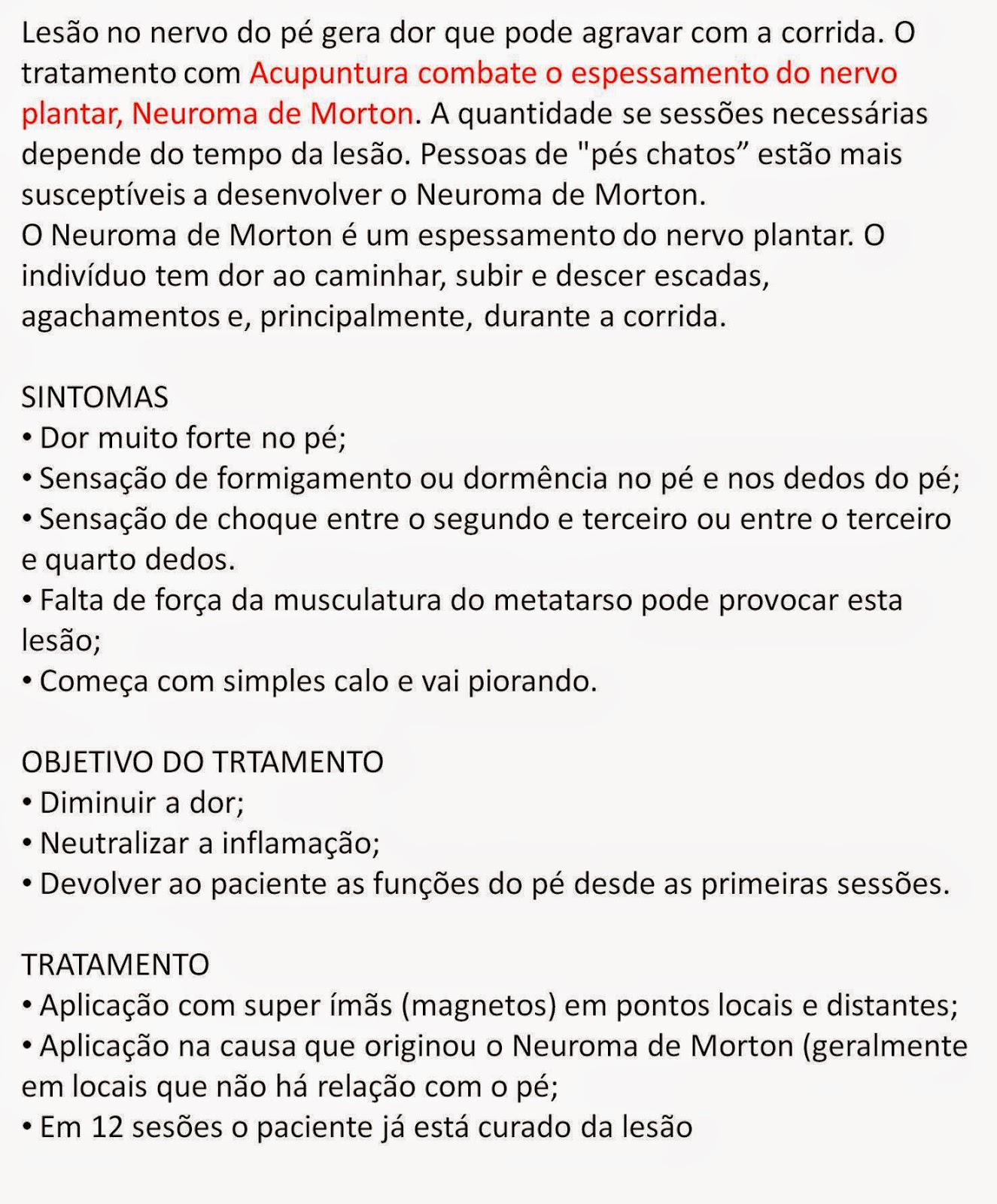 Surgical Treatment Operative treatment of Morton?s neuroma should be entertained only after failure of non-operative management. Standard operative treatment involves identifying the nerve and cutting (resecting) it proximal to the point where it is irritated/injured. This is usually done through an incision on the top (dorsal) aspect of the foot, although an incision on the sole (plantar) aspect of the foot can be used. Some physicians will attempt to treat Morton?s neuroma by releasing the intermetatarsal ligament, and freeing the nerve of local scar tissue. This may also be beneficial. There are actually not one but two unique variations of leg length discrepancies, congenital and acquired. Congenital indicates you are born with it. One leg is anatomically shorter than the other. Through developmental periods of aging, the brain picks up on the stride pattern and recognizes some variance. The human body usually adapts by dipping one shoulder to the "short" side. A difference of under a quarter inch is not blatantly irregular, demand Shoe Lifts to compensate and typically won't have a profound effect over a lifetime.
 Leg length inequality goes mainly undiscovered on a daily basis, however this problem is easily remedied, and can eradicate numerous incidents of back discomfort. Treatment for leg length inequality commonly involves Shoe Lifts. They are very reasonably priced, normally costing under twenty dollars, compared to a custom orthotic of $200 or higher. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position. Mid back pain is easily the most widespread condition affecting people today. Over 80 million people experience back pain at some stage in their life. It is a problem that costs businesses millions of dollars yearly due to lost time and production. Innovative and improved treatment methods are constantly sought after in the hope of lowering economical influence this issue causes.  People from all corners of the world experience foot ache as a result of leg length discrepancy. In most of these situations Shoe Lifts are usually of beneficial. The lifts are capable of alleviating any pain in the feet. Shoe Lifts are recommended by numerous specialist orthopaedic physicians. In order to support the body in a well balanced manner, your feet have a significant function to play. Irrespective of that, it's often the most overlooked zone in the human body. Some people have flat-feet which means there may be unequal force exerted on the feet. This causes other parts of the body such as knees, ankles and backs to be impacted too. Shoe Lifts guarantee that correct posture and balance are restored. There are actually two different kinds of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is structurally shorter in comparison to the other. Through developmental phases of aging, the brain senses the gait pattern and identifies some variance. The body usually adapts by dipping one shoulder over to the "short" side. A difference of less than a quarter inch isn't very irregular, does not need Shoe Lifts to compensate and generally doesn't have a profound effect over a lifetime.
 Leg length inequality goes largely undiagnosed on a daily basis, yet this issue is simply solved, and can eliminate quite a few cases of back ache. Treatment for leg length inequality typically consists of Shoe Lifts. These are generally very reasonably priced, frequently priced at under twenty dollars, in comparison to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Chronic back pain is the most common health problem afflicting men and women today. Around 80 million people have problems with back pain at some stage in their life. It is a problem which costs businesses millions year after year because of lost time and output. Fresh and more effective treatment methods are constantly sought after in the hope of reducing the economic influence this issue causes.  Men and women from all corners of the world suffer the pain of foot ache due to leg length discrepancy. In most of these situations Shoe Lifts are usually of beneficial. The lifts are capable of easing any pain in the feet. Shoe Lifts are recommended by many professional orthopaedic practitioners". So that they can support the body in a well-balanced manner, your feet have a very important function to play. Despite that, it is often the most overlooked zone in the body. Many people have flat-feet which means there is unequal force placed on the feet. This will cause other areas of the body including knees, ankles and backs to be affected too. Shoe Lifts guarantee that suitable posture and balance are restored.  Overview OverviewThe Hammertoes condition is usually irreversible, but often its progression can be slowed or halted. You should visit a Podiatrist if the toe becomes painful and you have difficulty walking. A Podiatrist will be able to provide advice and treatment including padding the bony top-part of your hammertoe to relieve pain or to tape your toes as a way to change their position. Podiatrists have an important role to play in preventing and managing foot problems. Prompt action is important. Problems which are left without assessment or treatment may result in major health risks. Causes Your shoes, your genetic predisposition, an underlying medical condition or all of these can make you susceptible to developing one of these deformities of the toes. The genes your parents gave you. When it comes to genetics, the foot type you?re born with predisposes you to developing this type of joint deformity over a lifetime. For many, a flat flexible foot leads to hammertoes as the foot tries to stabilize against a flattening arch. Those with high arches can also form hammertoes as the extensor tendons overpower the flexors.  Symptoms Pain upon pressure at the top of the bent toe from footwear. The formation of corns on the top of the joint. Redness and swelling at the joint contracture. Restricted or painful motion of the toe joint. Pain in the ball of the foot at the base of the affected toe. Diagnosis Your doctor is very likely to be able to diagnose your hammertoe simply by examining your foot. Even before that, he or she will probably ask about your family and personal medical history and evaluate your gait as you walk and the types of shoes you wear. You'll be asked about your symptoms, when they started and when they occur. You may also be asked to flex your toe so that your doctor can get an idea of your range of motion. He or she may order x-rays in order to better define your deformity. Non Surgical Treatment Padding and Taping. Often this is the first step in a treatment plan. Padding the hammertoe prominence minimizes pain and allows the patient to continue a normal, active life. Taping may change the imbalance around the toes and thus relieve the stress and pain. Medication. Anti-inflammatory drugs and cortisone injections can be prescribed to ease acute pain and inflammation caused by the joint deformity. Orthotic Devices. Custom shoe inserts made by your podiatrist may be useful in controlling foot function. An orthotic device may reduce symptoms and prevent the worsening of the hammertoe deformity. Surgical Treatment If conservative measures fail to provide relief, or if your hammertoe is in advanced stages with rigidity and a significant amount of pain, surgery may be required. Some patients also require surgery if they have open sores or wounds related to their hammertoe. For patients who also suffer from bunions, a combined procedure may be appropriate, addressing both conditions within the same surgery. Recovery time will vary from patient to patient, depending on the extent of the surgical repair and other conditions that may also be present. When a person has Hammer toes, the end of their toe bends downward and the middle joint curls up. Eventually, the toe gets stuck in a stiff, claw-like position. When the inside of your shoe rubs against a hammer toe, corns, blisters or calluses may form on top of the toe or on the bottom of your foot. This can make walking painful. You may also have pain in the joint where your big toe joins your foot. Hammer toe usually affects a person?s second toe (the toe next to the big toe), but it can affect other toes too. Causes Shoes that narrow toward the toe force the smaller toes into a bent upward position. This makes the toes rub against the inside of the shoe, and creates corns and calluses, aggravating the toes further. If the shoes have a high heel, the feet are forced forward and down, squeezing the toes against the front of the shoe, which increases the pressure on the toes and makes them bend further. Eventually, the toe muscles become unable to straighten the toe.  Symptoms The symptoms of hammertoe include a curling toe, pain or discomfort in the toes and ball of the foot or the front of the leg, especially when toes are stretched downward. Thickening of the skin above or below the affected toe with the formation of corns or calluses. Difficulty finding shoes that fit well. In its early stages, hammertoe is not obvious. Frequently, hammertoe does not cause any symptoms except for the claw-like toe shape. Diagnosis First push up on the bottom of the metatarsal head associated with the affected toe and see if the toe straightens out. If it does, then an orthotic could correct the problem, usually with a metatarsal pad. If the toe does not straighten out when the metatarsal head is pushed up, then that indicates that contracture in the capsule and ligaments (capsule contracts because the joint was in the wrong position for too long) of the MTP joint has set in and surgery is required. Orthotics are generally required post-surgically. Non Surgical Treatment Conservative treatment is the first choice, often starting with a change of shoes to ones that have soft, larger toe spaces. Toe exercises may be prescribed to stretch and strengthen the toe muscles. Over-the-counter straps, cushions or non-medicated corn pads may be recommended to help relieve your symptoms. Surgical Treatment Sometimes, if the deformity is severe enough or surgical modification is needed, the toe bones may be fused so that the toe does not bend. Buried wires are used to allow for the fusion to heal, and they remain in place after healing. Your skin is closed with fine sutures, which are typically removed seven to ten days after surgery. A dressing is used to help keep your toes in their new position. Dressings should not get wet or be removed. After surgery, your doctor may prescribe pain relievers, typically for the initial four to seven days. Most people heal completely within one month of surgery, with few complications, if any. Crutches or a cane may be needed to help you keep weight off your affected foot, depending on the procedure. Occasionally, patients receive a special post-op shoe or a walking boot that is to be worn during the healing process. Most people are able to shower normally after surgery, but must protect the dressing from getting wet. Many patients are allowed to resume driving within one week after the procedure, but care needs to be taken.
Overview
 A bunion (hallux valgus) is a deformity of the base joint of the big toe. The cause is not clear in many cases. The deformity may cause the foot to rub on shoes, which may cause inflammation and pain. Good footwear is often all that is needed to ease symptoms. An operation to correct the deformity is an option if good footwear does not ease symptoms. A bunion (hallux valgus) is a deformity of the base joint of the big toe. The cause is not clear in many cases. The deformity may cause the foot to rub on shoes, which may cause inflammation and pain. Good footwear is often all that is needed to ease symptoms. An operation to correct the deformity is an option if good footwear does not ease symptoms.Causes A bunion is more common in women than men due to women wearing tighter fitting shoes. This condition can cause a variety of different soft tissue and bony complaints which may result in severe pain. Symptoms Redness, swelling, or pain along the inside margin of the foot just behind the great toe. Moderate to severe discomfort at the bunion when wearing shoes, particularly if tight fitting. A painful callus may develop over the bunion. Sometimes a painful corn on the adjacent sides of the first and second toes. Irritation if there is overlapping of the first and second toes. Arthritis may cause stiffness and discomfort in the joint between the great toe and the first metatarsal. There may be a fluid filled cyst or bursa between the skin and the "bunion bone". Skin over the bunion may break down causing an ulceration, which can become infected. Diagnosis A thorough medical history and physical exam by a physician is necessary for the proper diagnosis of bunions and other foot conditions. X-rays can help confirm the diagnosis by showing the bone displacement, joint swelling, and, in some cases, the overgrowth of bone that characterizes bunions. Doctors also will consider the possibility that the joint pain is caused by or complicated by Arthritis, which causes destruction of the cartilage of the joint. Gout, which causes the accumulation of uric acid crystals in the joint. Tiny fractures of a bone in the foot or stress fractures. Infection. Your doctor may order additional tests to rule out these possibilities. Non Surgical Treatment Padding with a number of different materials (eg felt) to reduce pressure on the painful prominence of the bunion. Physical therapy can be used to help with the symptoms and improve the range of motion (this is particularly helpful if the pain is coming from inside the joint, rather than from shoe pressure). Manipulation of the joint can be used to help with this (manipulation will never correct the alignment of the joint). Any corns and calluses that are causing symptoms should be treated. The correct fitting of footwear is essential for anyone who is serious about doing something about their bunions and hallux valgus. It may be possible to have your shoes stretched over the area of the bunion to also relieve pressure. Foot orthotics may be useful in helping with the instability about the joint. They may be more helpful if there are other symptoms in the foot as well, as their use in "treating" bunions is controversial. They may play a role in slowing progression and in the prevention of bunions developing again after surgical correction. Exercises can be important in maintaining the mobility of the joint in those with bunions, this is especially important for the arthritic type pains that may be originating from inside the joint and for the prevention of these painful symptoms in the future.  Surgical Treatment There is more than one way to surgically treat a bunion. While there are some general guidelines, some procedures work well for some Surgeons and poorly for others. Your Surgeon should consider the severity of your bunion, medical condition, lifestyle, and recuperation time when considering the surgical treatment. Overview
n a normal functioning ankle and foot there should be 15- to 20-degrees of ankle dorsiflexion present (leg moving forward on top of the foot; or, same as the foot bending backward toward the leg) as well as 60- to 65-degrees of first toe extension (bending backward). Foot pronation (turning downward or inward) and supination (turning upward or outward) are normal and needed movements for proper function during the gait cycle. All feet must do this and do it well in order to minimize the forces that the body has to deal with during walking or running, and also to create the lever that is needed for propulsion.  Causes Although there are many factors that can contribute to the development of these conditions, improper biomechanics of the body plays a large and detrimental role in the process. Of the many biomechanical elements involved, foot and ankle function perhaps contribute the most to these aches and pains. Symptoms Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful. Diagnosis Your healthcare provider will ask about your symptoms, medical history, and activities and examine your feet. Your provider may watch you walk or run. Check the motion of your feet when they strike the ground. Look at your athletic shoes to see if they show an abnormal pattern of wear.  Non Surgical Treatment One of the best forms of treatment for over pronation is wearing supportive shoes. Shoes should have ample support and cushioning, particularly through the heel and arch of the foot. Without proper shoes, there may be additional strain on the tissue in the foot, greatly contributing to or causing an occurrence of over pronation. Rarely is surgery considered to relieve the pain and damage that may have resulted from this condition. Orthotic shoe inserts are often the easiest and most effective way to correct pronation. Prevention Pronation forces us to bear most of our weight on the inner border of our feet. Custom-made orthotics gently redistributes the weight so that the entire foot bears its normal share of weight with each step we take. The foot will not twist out at the ankle, but will strike the ground normally when the orthotics is used. This action of the custom-made orthotics will help to prevent shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, generalized fatigue, hammer toes, and calluses. |
